
Content verified by

What is spontaneous coronary artery dissection?
Spontaneous coronary artery dissection (SCAD) occurs when there is a tear or a bleed in the coronary artery wall, which disrupts the blood supply to the heart. This can weaken the heart and cause a medical emergency, such as cardiac arrest or heart attack, and should be treated urgently. It can happen suddenly with little or no symptoms.
If you suspect you or someone else is having a cardiac arrest or heart attack, it’s important to call 999 immediately.
Experts in treating women’s heart health
We’re proud to offer the only private SCAD service in the UK, with:
- a multi-disciplinary team of women’s health experts
- in-depth heart screening
- pre-conception heart screening and planning
- short-notice consultations, in as little as 24 hours

Symptoms of spontaneous coronary artery dissection
Symptoms of SCAD can include:
- chest pain or tightness
- dizziness or feeling lightheaded
- fatigue or feeling out of breath
- feeling hot, sweaty or clammy
- nausea
- tightness or pain in the arms, neck, jaw, back or stomach
SCAD can be misdiagnosed or ignored, as people often have no or very little cardiac risk factors or symptoms. Recovery following SCAD can be complex, patients should have a personalised plan to help them heal and adjust after a medical episode. Our specialists strongly encourage patients to seek investigations, post SCAD to assess potential risk factors, so these can be managed effectively.
If you want to discuss your heart health with one of our consultants, get in touch with our team to make an appointment.
What causes spontaneous coronary artery dissection?
The exact cause of SCAD is not fully understood. However, it has been linked to situations that put extra stress on blood vessels, especially if they’re already weakened or damaged.
These situations can include:
- extreme emotional stress
- pregnancy and birth
- vigorous physical exercise
Who is at risk of SCAD?
SCAD can affect anyone, but it is most common in healthy women aged 40–50 who have no traditional cardiovascular risk factors.
Risk factors for SCAD can include:
- autoimmune conditions: Conditions such as rheumatoid arthritis, lupus, Crohn’s disease, Hashimoto’s thyroiditis, and Graves’ disease can cause inflammation that may lead to arterial damage and weakness
- blood vessel disorders: Fibromuscular dysplasia causes abnormal growth of the artery walls, resulting in bead-like thickening or narrowing that can create weakness
- connective tissue disorders: Conditions such as Marfan syndrome can weaken the arterial walls, increasing the risk of tearing
- gender: Women are more likely to experience spontaneous coronary artery dissection, particularly during menopause
As there are currently no clear symptoms, our cardiac specialists are working hard to identify patients at the highest risk. Through heart screenings, including pre-conception heart checks and cardiac screening during the menopause, we can intervene before it develops into a medical emergency.
Complications of spontaneous coronary artery dissection
The complications of SCAD can be fatal, as small tears in the artery can prevent blood from flowing to the heart. This can weaken the heart, potentially leading to a SCAD heart attack. Some patients experience a separation of the inner and outer layers of their artery, causing blood to build up between the layers and worsening the condition.
Heart attacks caused by atherosclerosis are the result of cholesterol and plaque build-up, that causes narrowing or blocking of the arteries over time. In SCAD, the artery wall tears spontaneously, causing blood to pool within the wall layers and restrict blood flow. As SCAD damages the artery structure, patients may face a higher risk of ongoing complications such as recurrent tears or heart failure.
As many people with SCAD are asymptomatic, our consultants encourage women and those at risk to have a heart check and to monitor their blood pressure and cholesterol levels.
If you are concerned and would like to speak to one of our specialists, please contact our team to arrange an appointment.
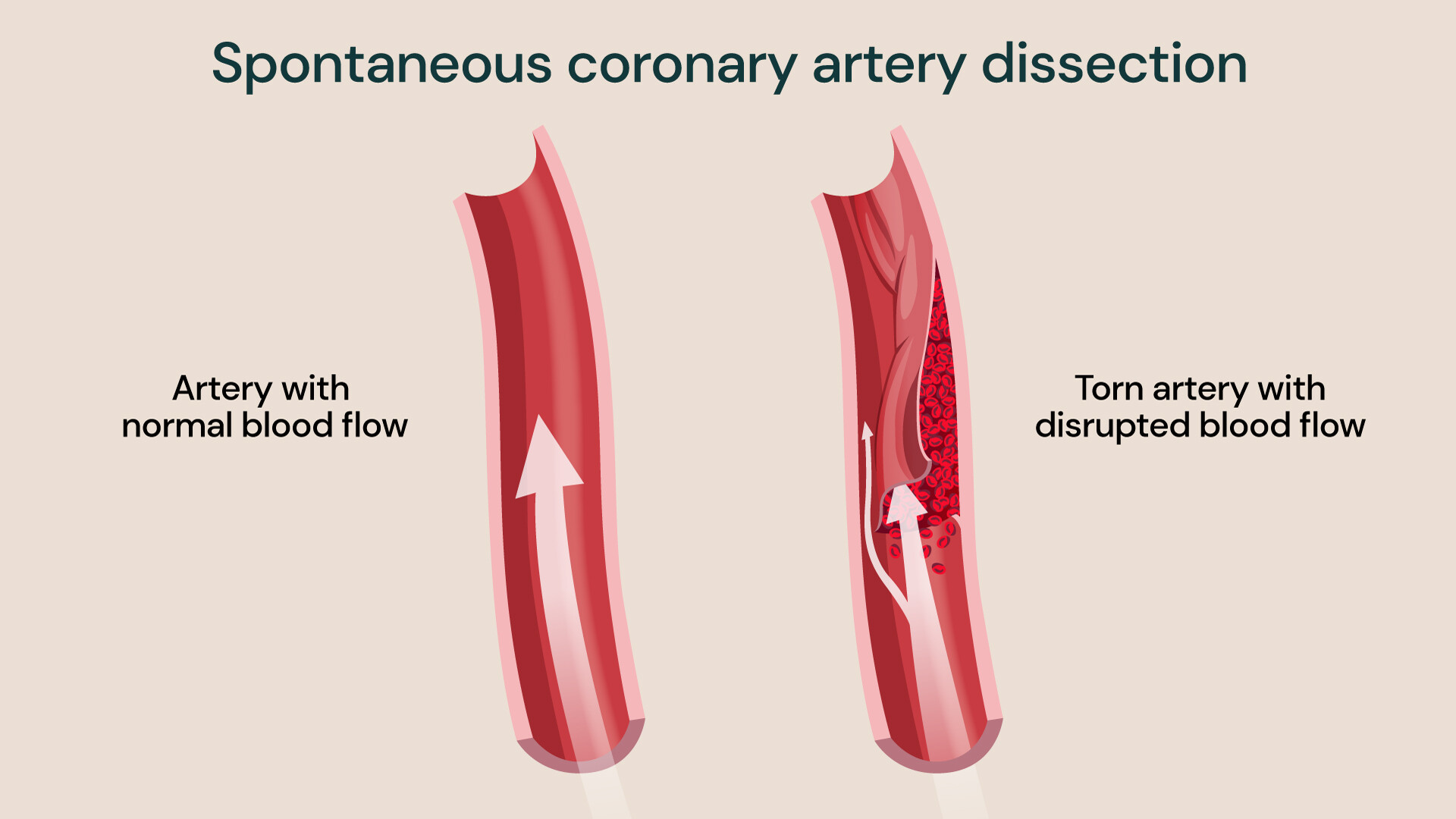
Visual representation of blood flow in arteries impacted by SCAD, illustrating how a tear can obstruct normal circulation.
Diagnosing spontaneous coronary artery dissection
SCAD can happen suddenly, and symptoms often go unnoticed. It doesn’t present with the same risk factors we usually associate with a heart attack, such as high cholesterol, high blood pressure, obesity, or smoking. In fact, people who experience SCAD are generally in good health.
Women, who are most affected by SCAD, signs and symptoms of women’s heart attack are less severe than those typically seen in men. These may include mild chest discomfort, nausea, fatigue, shortness of breath, or pain in the abdomen, neck, or jaw, which could be associated with other conditions or easily overlooked by patients.
Heart screening includes a series of tests that can be used to identify early signs of heart disease, even in patients who have no symptoms.
These tests include:
- blood tests
- coronary catheterisation (coronary angiogram)
- computerised tomography (CT) scan
- electrocardiogram (ECG)
Our world-leading cardiologists will use innovative investigations to make sure your heart is in the best possible health, while supporting you every step of the way with a personalised treatment plan if needed.
Spontaneous coronary artery dissection treatment
Treatment for SCAD is unique for each patient. An interventional cardiologist will develop a treatment plan based on the severity of your condition.
Common treatment options for SCAD include:
- coronary artery bypass grafting (CABG) to create a new pathway for blood to reach the heart muscle
- cardiac catheterisation (coronary angioplasty) and insertion of a stent to open the blocked artery and restore blood flow to the heart
- preventive medications to lower blood pressure and reduce the risk of blood clots
After treatment, we will support your recovery with a tailored cardiac rehabilitation programme, combining supervised exercise and lifestyle guidance, helping you live a fuller life with your heart condition.
Locations
Meet our team of expert cardiologists
Get help managing your risk of heart conditions like SCAD with the support of our world-leading cardiologists. We can provide a fast and accurate diagnosis and develop personalised treatment plans to manage your risks or condition.
Reviewed regularly to reflect clinical best practice
Last reviewed: 09 March 2026